Background:
The benefit of advanced life support measures in the management of patients with out-of-hospital cardiac arrest (OHCA) is controversial. Endotracheal intubation has long been considered the mainstay of definitive airway control in patients with cardiac arrest, however, there is a growing body of evidence to suggest that alternative airway interventions such as the implementation of supraglottic devices (i.e. laryngeal mask airways) may be of value. This is likely due to the ease in which these devices can be placed, and requirement for less training to obtain proficiency compared to endotracheal intubation. Studies looking at head to head comparisons of endotracheal intubation versus the use of supraglottic devices in OHCA are lacking. The primary goal of this study was to compare the difference in modified Rankin Scale (mRS) scores at hospital discharge or 30 days after OHCA in patients who were randomized to endotracheal intubation versus supraglottic device to see if supraglottic devices were superior.
Methods:
Between June 2015 and August 2017, the investigators conducted a multicenter, cluster randomized clinical trial involving 4 different ambulance services in England. Paramedics were randomized to use endotracheal intubation or supraglottic airways. In order to be included in the study, patients were required to meet the following criteria: 1) known or believed age greater or equal to 18; 2) non-traumatic OHCA; 3) treated by paramedic involved in study who was either first or second paramedic on scene; 4) continued resuscitation by EMS personnel. Patients were excluded from the study if they were prisoners, previously involved in the trial, had been deemed to have inappropriate resuscitation, had an advanced airway that was placed by another healthcare professional prior to arrival of study paramedics and patients that were known to be involved in other randomized control trials. The primary outcome of mRS score at discharge or 30 days after cardiac arrest was divided into favorable outcome (mRS score 0-3) or poor outcome (mRS score 4-6).
Key Results:
A total of 9.296 patients were enrolled in the trial, of which 4,886 patients were randomized to supraglottic airway versus 4410 were randomized to endotracheal intubation. The investigators presented the following important key findings:
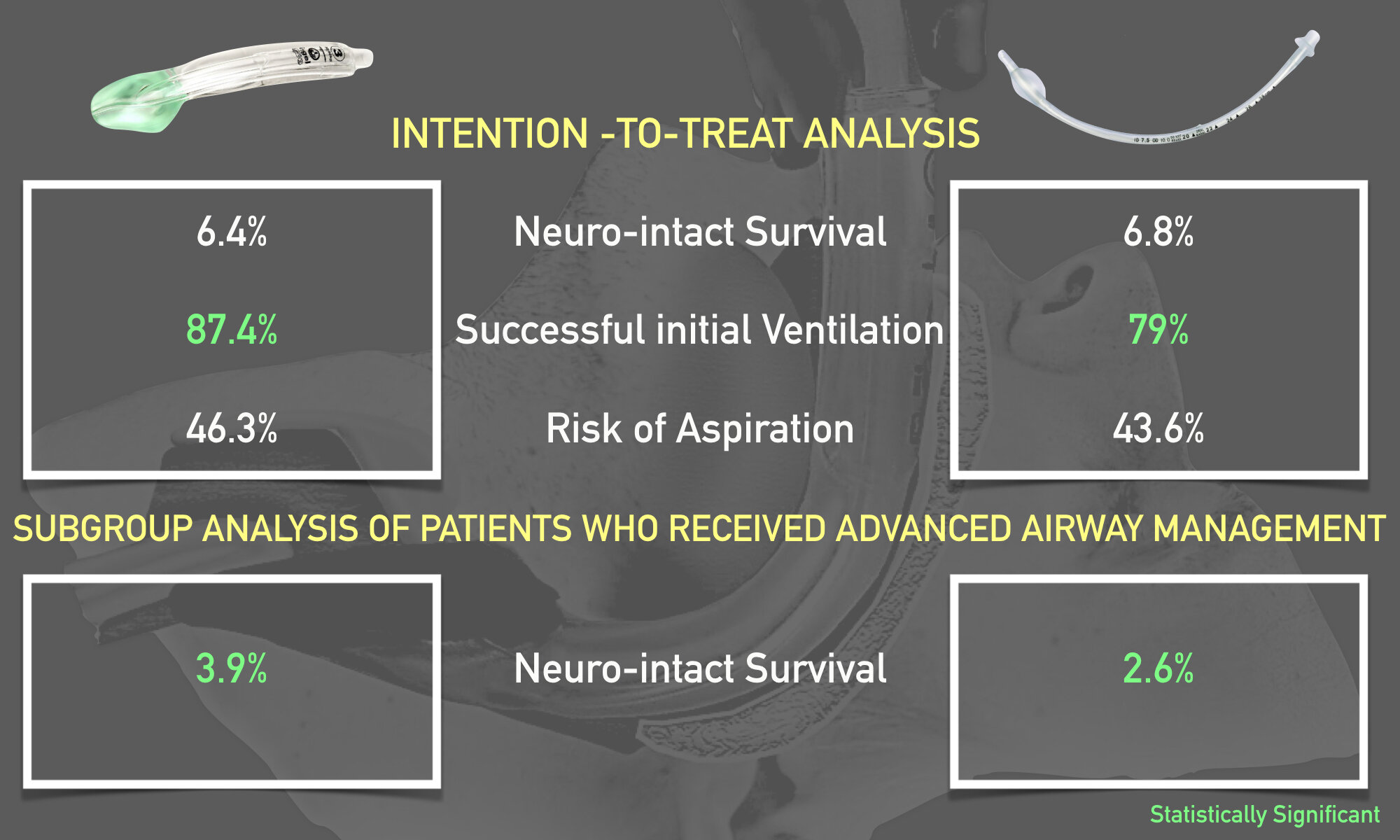
· Favorable neurologic outcome [ mRS score (0-3)] at 30 days or hospital discharge (whichever came first): 6.4% (311/4882) in the supraglottic airway group versus 6.8% (300/4407) in the endotracheal intubation group (adjusted risk difference -0.6%; 95% CI -1.6%-0.4%)
· In the subgroup analysis of 7576 patients who received advanced airway management (not intention-to-treat), more patients in the supraglottic airway device group had a favorable neurologic outcome (3.9%) vs. the tracheal intubation group (2.6%); risk difference, 2.1%; 95% CI, 1.2 – 2.9%
· Successful initial ventilation: 87.4% (4255/4868) in the supraglottic airway group versus 79.0% (3473/4397) in the endotracheal intubation group (adjusted risk difference 8.3%; 95%CI 6.3% to 10.2%).
· Rates of aspiration and regurgitation were not found to be different between the groups
Takeways:
Among patients with OHCA, advanced airway management with a supraglottic device was not associated with a favorable neurological outcome at 30 days compared to endotracheal intubation.
What This Means for EMS:
While the results of this study clearly indicated that advanced airway management with a supraglottic device was not associated with improvement in patient centered outcomes (in this case, neurological function), these devices were still associated with more successful initial ventilation without an increase in secondary complications such as aspiration/regurgitation. Furthermore, given the ease of use, less number of attempts required to obtain proficiency from a standpoint of training, and widespread availability, supraglottic devices are feasible intervention to provide airway support for patients with OHCA. Unlike endotracheal intubation which can be challenging to perform in the field with active chest compressions, supraglottic devices are easier to use in terms of temporary airway management and allow for the focus to be shifted towards measures that improve outcomes including high quality CPR and early defibrillation.
Article Bites Summary by Al Lulla, @al_lulla, Article Bites Editor